
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:22:038 | Recurrent Pneumonias and Persistent Inflammation in VEXAS Syndrome: The Role of BAL in Differential Diagnosis
Francesco Ghellere1, Bernardo D'Onofrio1, Maria Chiara Ditto1, Salvatore Panaro1, Francesca Piccione1|2, Giacomo Tanti1, Enrico Fusaro1, Simone Parisi1 | 1SC Reumatologia, Città della Salute e della Scienza Torino, Italy; 2Fondazione Ricerca Molinette Torino, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
68
Views
Authors
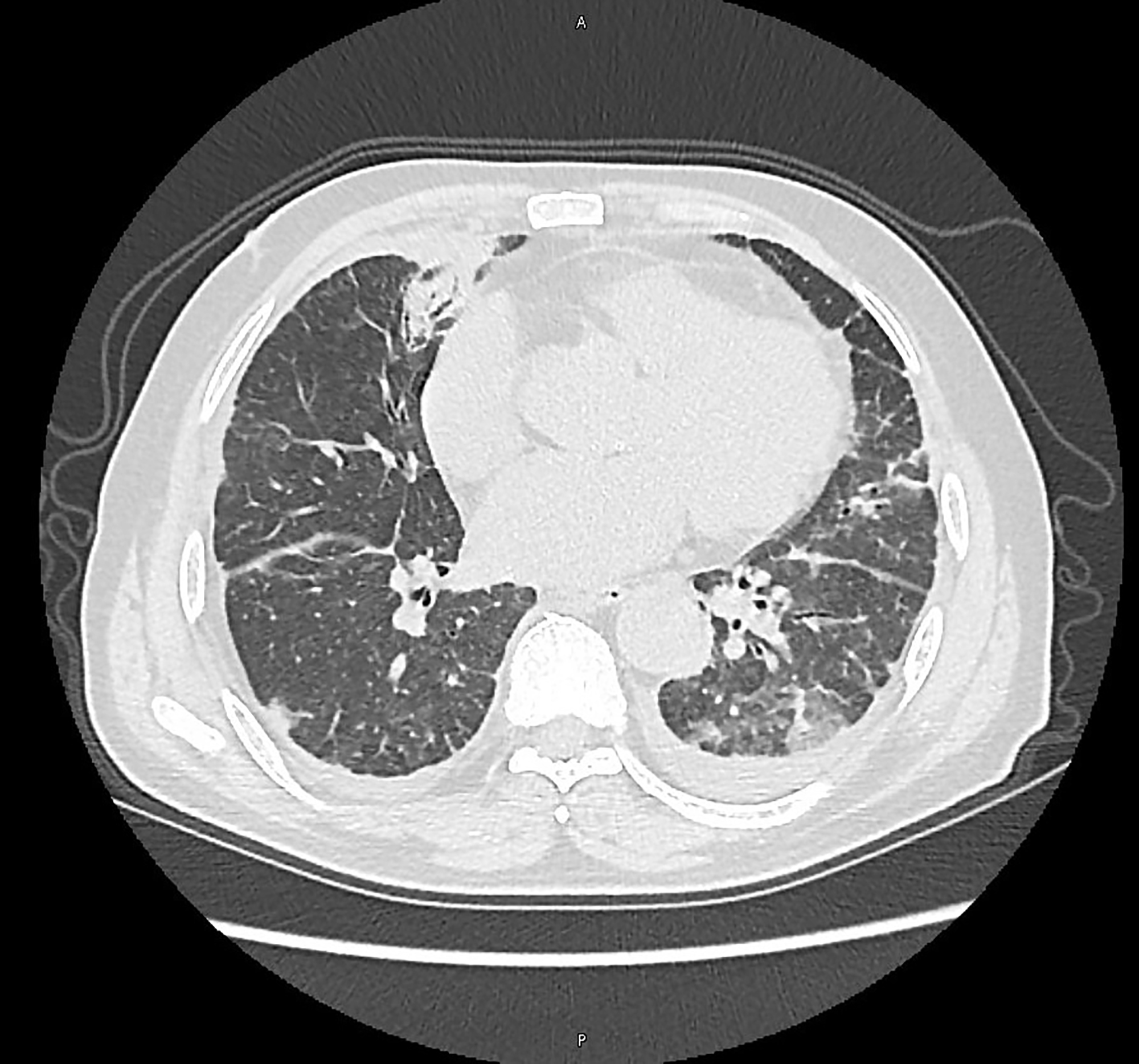
Methods. A patient with recent diagnosis of VEXAS syndrome under treatment with Tocilizumab (IV) and corticosteroids was hospitalized for pleuritic chest pain, fever, and CT evidence of bilateral peribronchial consolidations and pleural effusion. Laboratory tests showed marked neutrophilic leukocytosis and elevated CRP (242 mg/L) with normal procalcitonin. Given the history of recurrent pneumonias and immunosuppression, an extensive infectious workup was initiated, including BAL with microbiological and immunocytological analysis.
Results. BAL was negative for bacteria, fungi, viruses, and mycobacteria (culture, PCR panel, antigen testing, serologies, and staining). Cytological analysis revealed a CD4+ T-cell predominant lymphocytic response, reduced macrophages, absence of B-cells, and normal NK cell counts. Lack of improvement with antibiotics and rapid clinical response to intravenous corticosteroids led to the diagnosis of inflammatory lung involvement. The patient showed rapid defervescence, CRP reduction (<10 mg/L), and radiological resolution of consolidations.
Conclusions. This case highlights the importance of an integrated clinical and immunological approach in evaluating pulmonary symptoms in VEXAS syndrome. In this patient the history of recurrent pneumonias could indicate pulmonary involvement of VEXAS syndrome even prior to the onset of rheumatological symptoms. BAL cytology, combined with microbiological exclusion and clinical response to therapy, can differentiate inflammatory flares from infectious pneumonia. According to literature, it affects approximately 34% of VEXAS patients (Beck DB et al., NEJM 2020), often presenting with non-specific consolidations or vasculitis. In this complex patient group, BAL-guided management is crucial to avoid unnecessary antibiotics and promptly initiate immunosuppressive therapy.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:22:038 | Recurrent Pneumonias and Persistent Inflammation in VEXAS Syndrome: The Role of BAL in Differential Diagnosis: Francesco Ghellere1, Bernardo D’Onofrio1, Maria Chiara Ditto1, Salvatore Panaro1, Francesca Piccione1|2, Giacomo Tanti1, Enrico Fusaro1, Simone Parisi1 | 1SC Reumatologia, Città della Salute e della Scienza Torino, Italy; 2Fondazione Ricerca Molinette Torino, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Aug. 7];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2346
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


