
PO:25:073 | Pulmonary involvement and progressive interstitial lung disease in anti-synthetase syndrome: a single-center retrospective study
Daniele Scaramuzzi1|3, Giacomo De Luca1|3, Veronica Batani1, Giulia Buonsante1|3, Lorenzo Dagna1|3, Marco Matucci-Cerinic1|2|3, Corrado Campochiaro1|2|3 | 1Unità di Immunologia, Reumatologia, Allergologia e Malattie Rare, IRCCS Ospedale San Raffaele, Milano; 2Inflammation, Fibrosis and Ageing Initiative INFLAGE, IRCCS San Raffaele Hospital, Milano; 3Università Vita-Salute San Raffaele, Milano, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background. Anti-synthetase syndrome (ASS) is a systemic autoimmune disease frequently associated with lung involvement. This single-center retrospective study aimed to longitudinally assess the clinical and instrumental evolution of patients with ASS and Interstitial Lung Disease (ILD) and to evaluate the rate of disease progression.
Materials and Methods. Clinical and instrumental data, including spirometric parameters (%pFVC and %pDLCO), radiological patterns, and fibrotic extent according to HRCT visual scoring, were collected at three time points: baseline (first visit at our center), 12 ± 3 months, and 24 ± 3 months. Progressive ILD at 12 and 24 months was defined according to the ATS/ERS/JRS/ALAT 2022 guidelines (presence of at least two among worsening respiratory symptoms, decline in %pFVC ≥ 5% or in %pDLCO ≥ 10%, or radiological progression) and the INBUILD trial criteria (at least one among %pFVC decline ≥ 10%, 5–10% decline in %pFVC with worsening symptoms or radiological progression, or worsening of symptoms and radiological progression). Predictors of progression were analyzed.
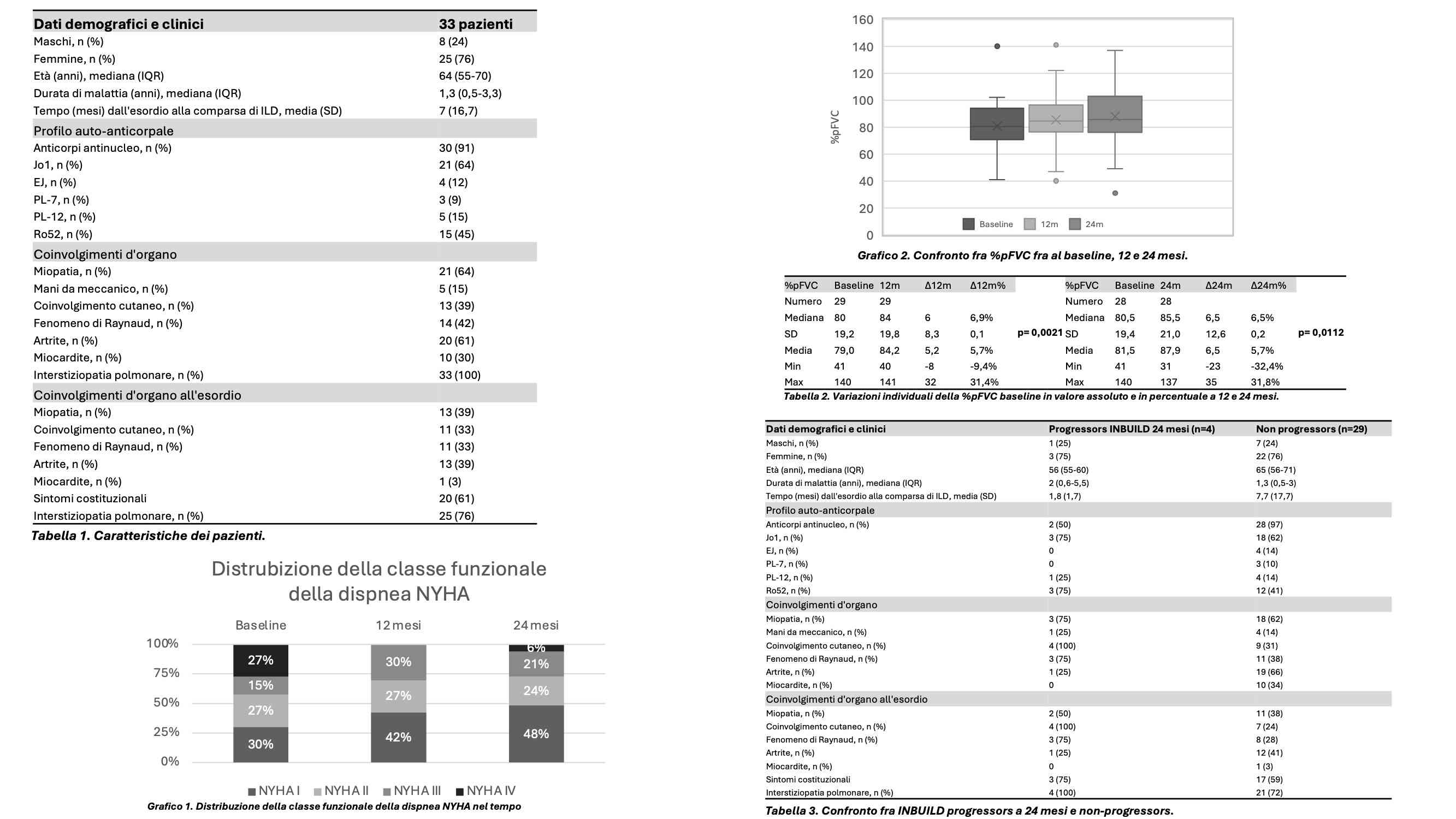
Results. Thirty-three patients with ASS-ILD were included. Patients and disease characteristics are summarized in Table 1. Twenty-five patients (76%) presented pulmonary involvement at disease onset. The most frequent radiological pattern was NSIP, observed in 23 patients (70%), followed by UIP in 6 patients (18%), OP in 2 patients (6%), and mixed NSIP-OP in 2 patients (6%). Fibrotic extent on HRCT was ≤10% in 15 patients (46%), 10–20% in 10 patients (30%), and >20% in 8 patients (24%). The distribution of NYHA functional class for dyspnea across the three time points is shown in Graphic 1. We observed an improvement from baseline in NYHA functional class for dyspnea (2, 4, and 2 patients moved from class IV, III, and II to class I, respectively, at both 12 and 24 months), as well as an improvement in exertional dyspnea at 24 months [24 (73%) vs 15 (45%); p = 0.0242], together with a progressive increase in %pFVC values at the two time points (Graphic 2, Table 2). Five (15%) and four (12%) patients were classified as progressors at 12 and 24 months, respectively. The characteristics of patients with INBUILD-defined progression at 24 months compared with those without progression are summarized in Table 3. No predictor of ILD progression was identified.
Conclusions. In our cohort of patients with ASS-ILD, the %pFVC and NYHA functional classes improved over 12 and 24 months of follow-up. The proportion of progressors identified according to the two criteria was reduced (15% and 12%). No predictor of progression was identified.

Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


