
PO:32:176 | Outcomes of upfront combination vs monotherapy with rituximab or mycophenolate mofetil for systemic sclerosis interstitial lung disease: results from a European Scleroderma Trials and Research cohort study
Devis Benfaremo1, Corrado Campochiaro2, Gábor Kumánovics3, Christina Bergmann4, Elisabetta Zanatta5, David Launay6, Serena Guiducci7, Mickael Martin8, Carolina De Souza Müller9, Carlomaurizio Montecucco10, Luc Mouthon11, Gabriella Szucs12, Kastriot Kastrati13, Marie-Elise Truchetet14, Madelon Vonk15, Francesco Del Galdo16, Marco Matucci-Cerinic2, Gianluca Moroncini1, Yannick Allanore17. | 1Department of Clinical and Molecular Sciences, Marche Polytechnic University, Marche University Hospital, Ancona, Italy; 2Vita-Salute San Raffaele University, San Raffaele Hospital, Milano, Italy; 3University of Pécs, Department Of Rheumatology And Immunology, Pécs, Hungary; 4University Hospital Erlangen, Department Internal Medicine 3, Erlangen, Germany; 5Padova University Hospital, Rheumatology Unit, Padova, Italy; 6Univ. Lille, Inserm, CHU Lille, Department of Internal Medicine and Clinical Immunology, Lille, France; 7University of Florence, Azienda Ospedaliera Universitaria Careggi, Firenze, Italy; 8Poitiers University Hospital, Department of Internal Medicine Poitiers France; 9Hospital de Clinicas da Universidade Federal do Parana Curitiba Brazil; 10Università di Pavia e IRCCS Fondazione Policlinico S. Matteo, Pavia, Italy; 11Hôpital Cochin, Department of Internal Medicine, Paris, France; 12University of Debrecen, Faculty of Medicine, Department of Rheumatology, Debrecen, Hungary; 13Medical University of Vienna, Department of Medicine III, Division of Rheumatology, Vienna, Austria; 14CHU de Bordeaux, Rheumatology department, Bordeaux, France; 15Radboudumc, Department of Rheumatology Nijmegen The Netherlands; 16Leeds Raynauds and Scleroderma Program, NIHR Biomedical Research Centre, Leeds, United Kingdom; 17Université Paris Cité, Cochin Hospital, Rheumatology Department, Paris, France.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background. Interstitial lung disease (ILD) is a major complication in systemic sclerosis (SSc) patients as it is associated with increased mortality and significant morbidity. Since combination therapies are foreseen as the future of SSc-ILD management, in this study we aimed to compare the outcomes at 12 months in patients with SSc-ILD treated with RTX alone, MMF alone, or upfront combination therapy (MMF + RTX).
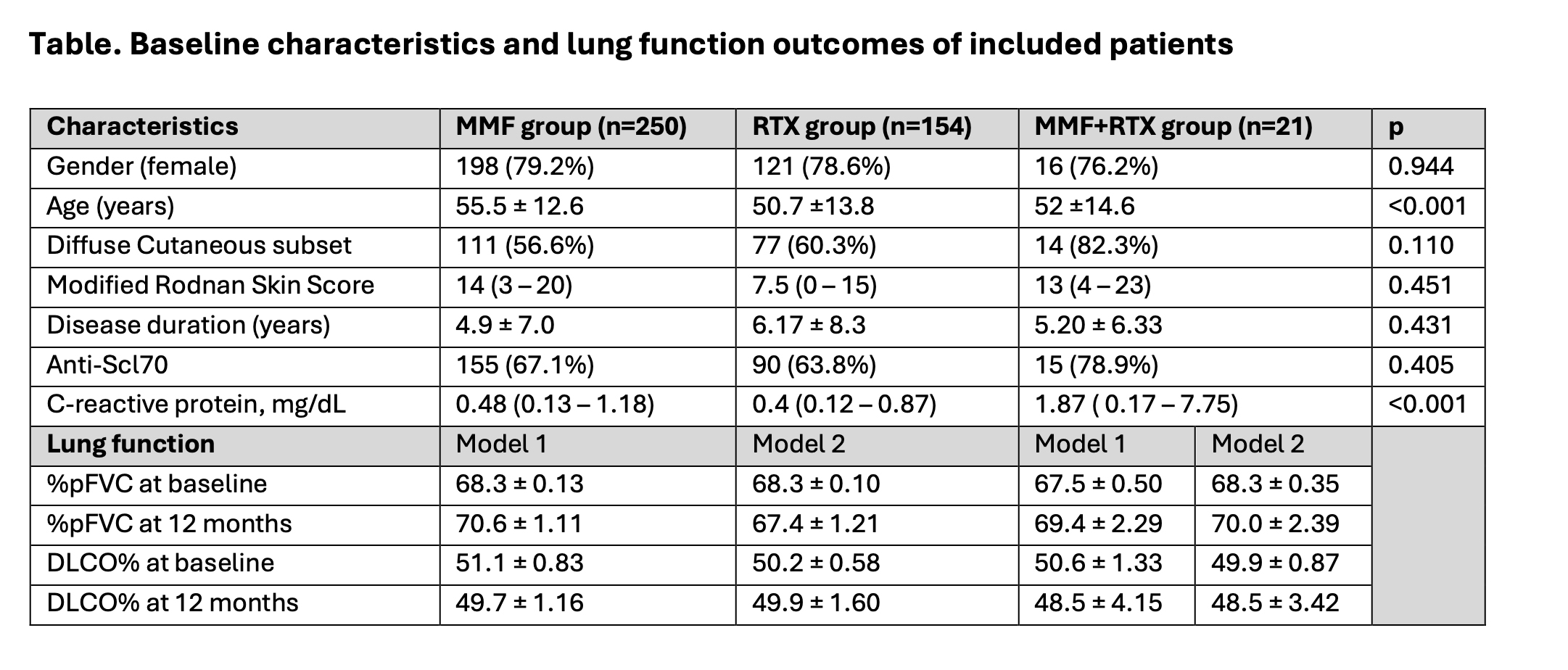
Materials and Methods. SSc patients meeting the 2013 ACR/EULAR criteria, with ILD confirmed by chest HRCT and available % predicted FVC (%pFVC) at baseline and 12 ± 3 months, were eligible for inclusion. Patients were grouped based on treatment initiated at baseline: (a) MMF alone, (b) RTX alone, or (c) upfront combination therapy (MMF + RTX). Patients on nintedanib or tocilizumab at baseline were excluded. Inverse probability of treatment weighting (IPTW) was used to adjust for confounding and treatment imbalances, following multiple imputation for missing data. Propensity score models incorporated the following variables: age, gender, disease subset (diffuse vs. limited), autoantibody status (ATA positivity), baseline FVC, and disease duration. Linear mixed-effects models were used to compare the change in %pFVC and DLCO% at 12 ± 3 months across groups. The proportion of patients with ILD progression (FVC decline >5%) was also estimated.
Results. A total of 425 patients were included in the final analysis (250 MMF, 154 RTX and 21 combination therapy). At 12 months, FVC remained stable in all treatment groups. In model 1 (MMF vs. combination), the mean change in FVC was 2.28% (95%CI 0.10 — 4.40) for MMF vs 1.83% (95%CI -2.8 — 6.5) for the combination group (mean difference -0.44, 95%CI -5.70 — 4.80, p = 0.867). The mean change in DLCO was -1.35% (95%CI -3.92 — 1.21) for MMF vs -2.05% (95%CI -11.2 — 7.14) for the combination group (mean difference -0.7, 95%CI -10.0 — 8.61, p = 0.882). In model 2 (RTX vs. combination), the mean change in FVC was -0.93% (95%CI -3.29 — 1.43) for RTX vs 1.71% (95%CI -2.97 — 6.41) for the combination group (mean difference 2.65, 95%CI -2.52 — 7.82, p = 0.315). The mean change in DLCO was -0.35% (95%CI -3.48 — 2.78) for RTX vs -1.43% (95%CI -8.6 — 5.73) for the combination group (mean difference -1.08, 95%CI -8.71 — 6.54, p = 0.781). The proportion of patients with ILD progression at 12 months was similar across treatment groups: MMF 29.2% (95%CI 23.3-35.1), RTX 28.1% (95%CI 20.2-36.0), and combination therapy 27.4% (95%CI 5.9-48.8).
Conclusions. This EUSTAR cohort analysis does not demonstrate a clear benefit of upfront combination therapy with MMF and RTX over treatment with either agent alone regarding FVC decline at 12 months in SSc-ILD patients.

Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


