
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:35:234 | Sustained Vasculitis Quiescence and CS Reduction with Mepolizumab 100 mg
Francesca Mascia1, Angelo Fassio2, Marco Zurlo1, Davide Chesini3, Francesco Pollastri2, Giovanni Adami2, Davide Gatti4, Maurizio Rossini4, Matteo Maule5, Gianentrico Senna1, Marco Caminati1 | 1University of Verona - Allergology and Clinical Immunology Verona, Italy; 2Policlinico G. B. Rossi - Rheumatology Verona, Italy; 3University of Verona - Faculty of Medicine and Surgery Verona, Italy; 4University of Verona - Rheumatology Verona, Italy; 5Policlinico G. B. Rossi - Allergology and Clinical Immunology Verona, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
41
Views
Authors
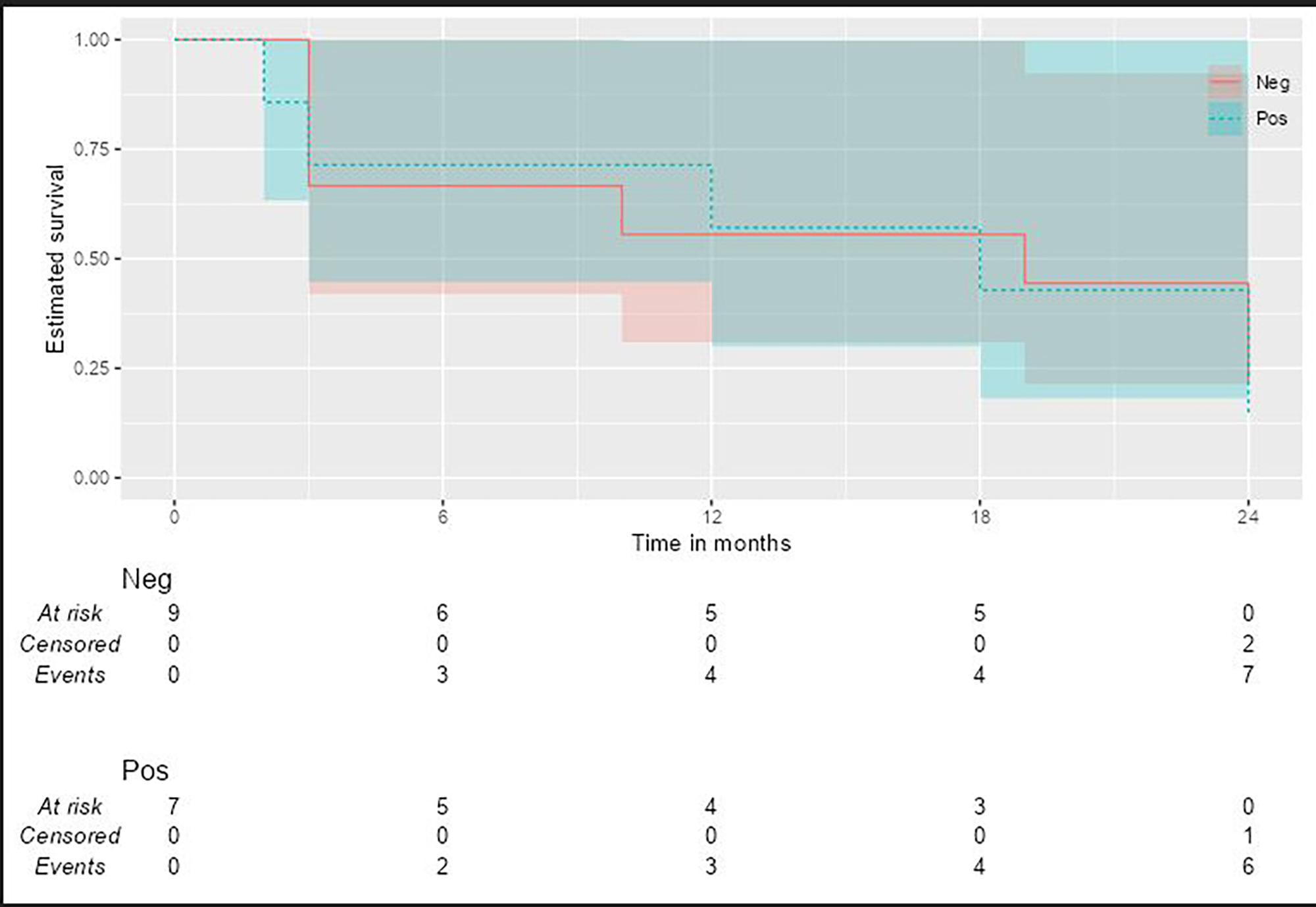
Objective and Methods. In this single-centre observational study at the University Hospital of Verona we aimed to assess the long-term efficacy, safety and CS/IS-sparing impact of mepolizumab 100 mg monthly in EGPA patients whose vasculitis was quiescent but who continued to experience refractory eosinophilic asthma. We enrolled 36 patients meeting ACR criteria for EGPA, with severe steroid-dependent asthma and Birmingham Vasculitis Activity Score (BVAS)–confirmed remission, received mepolizumab 100 mg every four weeks. Clinical data were retrospectively collected at disease onset, at treatment initiation (baseline), and at 6, 12, 18 and 24 months. We recorded BVAS, daily prednisone dose, concomitant IS use, peripheral eosinophil count, ANCA status, FEV1 % predicted, fractional exhaled nitric oxide (FeNO), Asthma Control Test (ACT) scores, asthma exacerbations and hospitalizations. Repeated measures ANOVA evaluated parameter trends over time. A Cox proportional hazards model examined whether baseline BVAS, prednisone dose or ANCA status predicted time to IS discontinuation. Remission at 24 months was defined per MIRRA criteria as BVAS = 0 with prednisone < or = 4 mg/day.
Results and Conclusions. At baseline, no patient met remission criteria, by months 12 and 24, 10 of 36 patients achieved remission, with no significant difference between ANCA-positive and ANCA-negative subgroups. BVAS and eosinophil counts declined significantly (p < 0.001). Median daily prednisone fell from approximately 50 mg at baseline to < or = 4 mg, enabling 75% of patients to discontinue corticosteroids by 24 months. ACT scores improved, FeNO levels declined and FEV1 remained stable. Rates of asthma exacerbation and hospitalization approached zero. Six patients (14%) required dose escalation to 300 mg or switching biologic due to flares. In Cox regression, higher baseline BVAS was associated with a lower likelihood of IS discontinuation (HR 0.87; 95% CI, 0.78–0.97; p = 0.014). Mepolizumab 100 mg monthly led to sustained reductions in vasculitis activity, eosinophil counts and CS/IS requirements, supporting an “asthma-tailored” low-dose strategy for EGPA patients in remission. Future multicenter randomized trials and biomarker studies are necessary to optimize patient selection and dosing strategies for long-term management.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:35:234 | Sustained Vasculitis Quiescence and CS Reduction with Mepolizumab 100 mg: Francesca Mascia1, Angelo Fassio2, Marco Zurlo1, Davide Chesini3, Francesco Pollastri2, Giovanni Adami2, Davide Gatti4, Maurizio Rossini4, Matteo Maule5, Gianentrico Senna1, Marco Caminati1 | 1University of Verona - Allergology and Clinical Immunology Verona, Italy; 2Policlinico G. B. Rossi - Rheumatology Verona, Italy; 3University of Verona - Faculty of Medicine and Surgery Verona, Italy; 4University of Verona - Rheumatology Verona, Italy; 5Policlinico G. B. Rossi - Allergology and Clinical Immunology Verona, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Jul. 28];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2387
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


