
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:31:171 | Uncovering subclinical cardiac involvement in VEDOSS: An echocardiographic driven study
Eugenio Capparelli1, Eleonora Zaccara1, Irene Rota2, Sara Facetti2, Daniela Bompane1, Laura Castelnovo1, Antonino Mazzone3, Paola Faggioli1 | 1UOC Reumatologia, ASST Ovest-Milanese, Legnano Milano Italy; 2UOC Cardiologia, ASST Ovest-Milanese, Legnano Milano, Italy; 3UOC Medicina Interna, ASST Ovest-Milanese, Legnano, Milano, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
35
Views
Authors
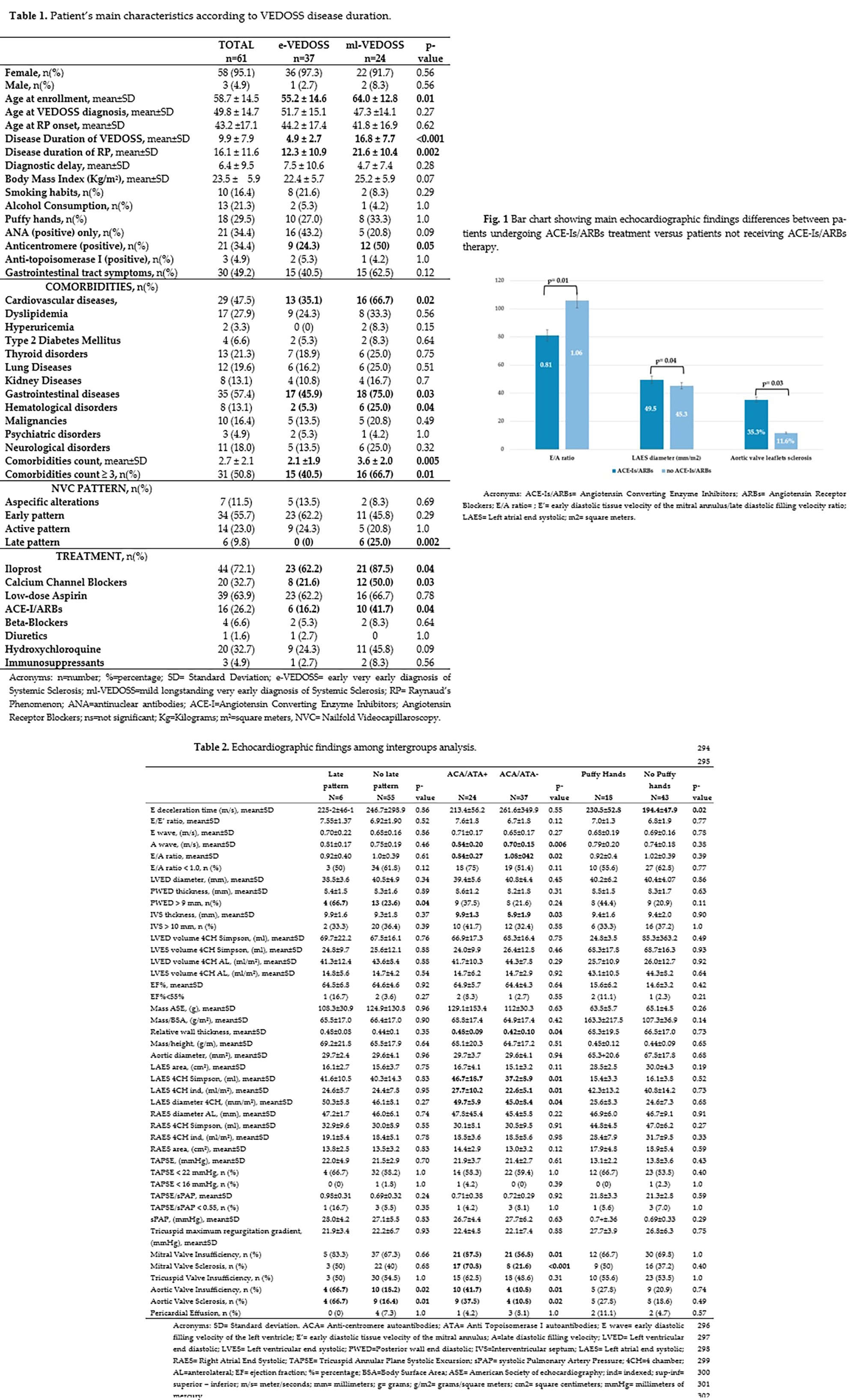
Methods. We conducted a cross-sectional observational study involving 61 patients meeting VEDOSS criteria followed up regularly within our Scleroderma Unit. Patients were categorized as early VEDOSS (eVEDOSS, n=37) or mild-longstanding VEDOSS (mlVEDOSS, n=24) based on disease duration (more than 10 years). We analyzed clinical and demographic data, focusing on echocardiographic parameters such as the E/A ratio, as indicative of left ventricular diastolic dysfunction (LVDD) and interventricular septum (IVS) and posterior wall at end diastole (PWED) thicknesses for LV systolic dysfunction (LVSD). Areas and dimensions of both atriums were also assessed. Statistical analyses included Chi-square and Student's T tests, with a significance threshold of p<.05.
Results. Higher comorbidities burden was found in patient with longer disease duration (ml-VEDOSS), specifically cardiovascular, hematological and gastrointestinal disorders (Table 1). Ml-VEDOSS patients presented also with a greater prevalence of anti-centromere antibodies positivity compared to e-VEDOSS. However, no differences emerged for LVDD and LVSD comparing ml-VEDOSS and e-VEDOSS patients, while patients exhibiting SSc specific autoantibodies positivity exhibited lower E/A ratios and increased left atrial (LA) size (Table 2). Late nailfold videocapillaroscopic pattern patients exhibited increased PWED thickening and aortic valve insufficiency. Notably, patients undergoing Iloprost iv administration only experienced larger right atrial (RA) volume measured in the superior-inferior direction at end-systole (18.1±5.1 mm/m2), while further increasing in patients receiving both Iloprost and CCBs (21.7±4.5 mm/m2), compared to patients receiving no vasodilators (16.6±2.1 mm/m2). Renin-Angiotensin-Aldosterone System (RAAS) inhibitors patients reported reduced E/A ratio (p=0.01) and larger LA diameter measured in the superior-inferior direction at end-systole (49.5±5.8 vs 45.3±8.4 mm/m2, p=0.04) and a greater prevalence of aortic valve leaflets sclerosis (35.3% vs 11.6%, p=0.03) (Fig 1). E/A ratios, PWED and IVS thickening were included in multiple general regression model as independent variables. Multivariable regression analysis confirmed DLCO% as the sole predictor of both LVDD and LVSD in VEDOSS population.
Conclusions. Careful monitoring of cardiac function in VEDOSS patients is crucial as alterations may occur even in the absence of symptoms. DLCO% emerged as an important predictor of both LVDD and LVSD.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:31:171 | Uncovering subclinical cardiac involvement in VEDOSS: An echocardiographic driven study: Eugenio Capparelli1, Eleonora Zaccara1, Irene Rota2, Sara Facetti2, Daniela Bompane1, Laura Castelnovo1, Antonino Mazzone3, Paola Faggioli1 | 1UOC Reumatologia, ASST Ovest-Milanese, Legnano Milano Italy; 2UOC Cardiologia, ASST Ovest-Milanese, Legnano Milano, Italy; 3UOC Medicina Interna, ASST Ovest-Milanese, Legnano, Milano, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Aug. 2];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2369
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


