
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:31:161 | First-line diagnostic tests to intercept primary heart involvement in systemic sclerosis: clinical associations from the SPRING-SIR registry
Antonio Tonutti1|2, Francesca Motta1|2, Rossella De Angelis3, Valeria Riccieri4, Silvia Laura Bosello5, Fabio Cacciapaglia6, Veronica Codullo7, Giacomo De Luca8, Francesca Ingegnoli9, Dilia Giuggioli10, Clodoveo Ferri10, Marco Matucci-Cerinic8, Carlo Selmi1|2, Maria De Santis1|2 | 1Department of Biomedical Sciences, Humanitas University Pieve Emanuele, Milan, Italy; 2Rheumatology and Clinical Immunology, IRCCS Humanitas Research Hospital Rozzano, Milan, Italy; 3Università Politecnica delle Marche Ancona, Italy; 4Università degli Studi di Roma La Sapienza Roma, Italy; 5Università Cattolica del Sacro Cuore Roma, Italy; 6Università degli Studi di Bari Aldo Moro Bari, Italy; 7Reumatologia, Fondazione IRCCS Policlinico San Matteo Pavia, Italy; 8Università Vita-Salute San Raffaele Milano, Italy; 9Università degli Studi di Milano, Italy; 10Università degli Studi di Modena e Reggio Emilia, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
86
Views
Authors
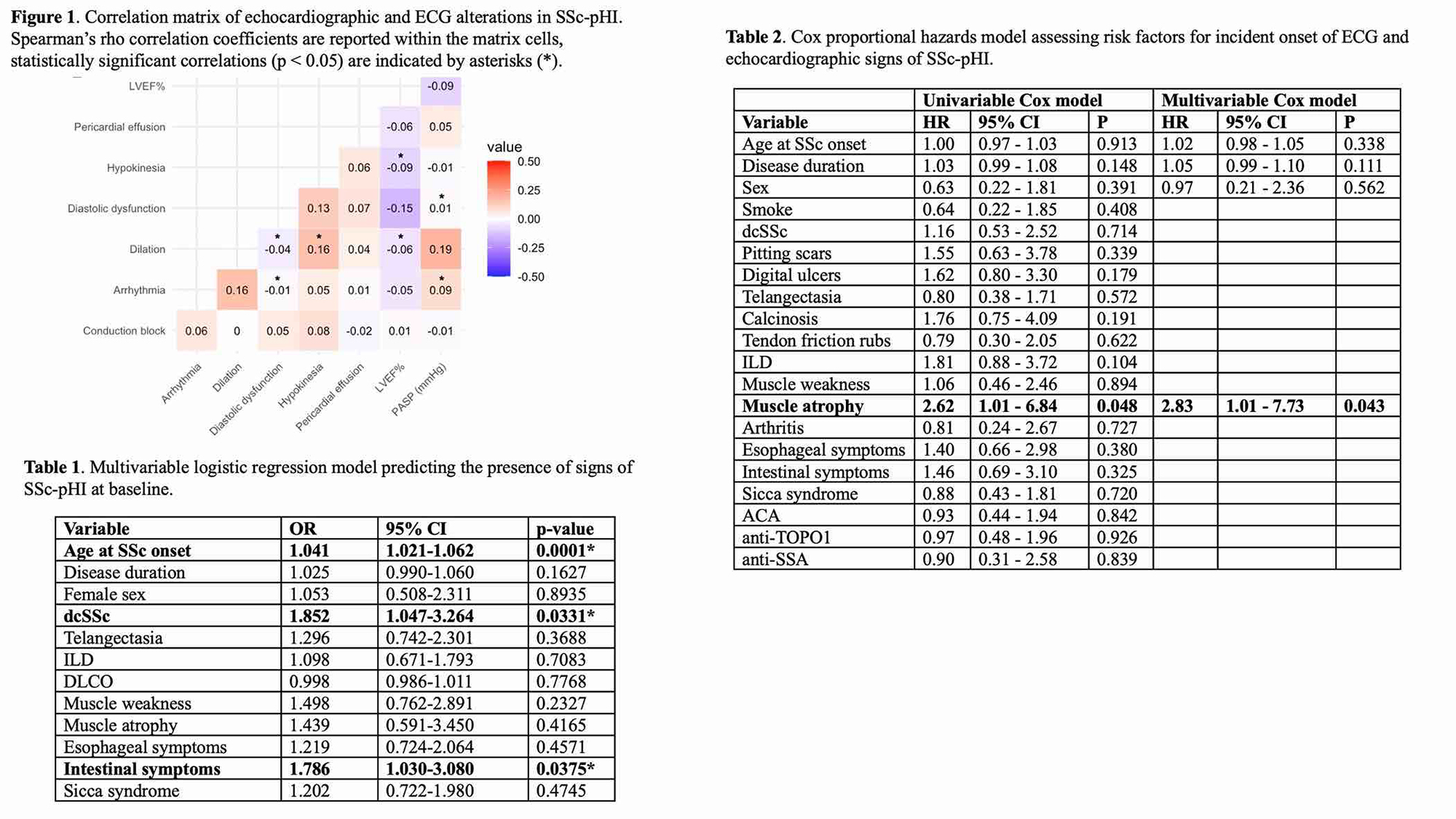
Results. Of 600 eligible patients, 90% were females, with a median age at SSc onset of 45 (IQR 35-55) and disease duration of 8 years (4-14); 22% had dcSSc, 43% ILD, 24% digital ulcers, 16% muscle weakness, 6.5% muscle atrophy, 53% esophageal and 22% intestinal involvement. Anti-Scl70 were positive in 41%, ACA in 39%. At baseline, 149 (25%) had signs of SSc-pHI. Diastolic dysfunction was the most common alteration (62%), followed by conduction block (34%), arrhythmia (11%), LV dilation (9%), and hypokinesia (3%). The alterations were not mutually exclusive. Weak but significant correlations were found between increasing PASP and arrhythmia, increasing PASP and diastolic dysfunction, and LV dilation and non-ischemic hypokinesia; diastolic dysfunction negatively correlated with LV dilation and arrhythmia (Figure 1). In the multivariable logistic regression (adjusted for age, sex, and duration), the risk of SSc-pHI was increased with dcSSc (OR 1.85; 95%CI 1.05-3.26), intestinal symptoms (OR 1.79; 95%CI 1.03-3.08), and age at SSc onset (OR 1.04; 95%CI: 1.02-1.06) (Table 1). During follow-up (data available for 125 subjects), 31 new SSc-pHI cases were recorded (cumulative incidence 25%). Overall mortality did not differ between patients with or without incident SSc-pHI. Cox proportional hazards regression (adjusted for age, duration, and sex) revealed muscle atrophy as the only risk factor for new-onset SSc-pHI (HR 2.83, 95%CI 1.01-7.73) (Table 2). Exposure to immunosuppressive and vasoactive treatments did not differ between patients with or without SSc-pHI.
Conclusions. pHI is a protean and severe complication possibly affecting one-quarter of SSc cases. Early detection is crucial, and patients older at disease onset, with the diffuse form, muscular involvement, and intestinal manifestations can be those at higher risk.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:31:161 | First-line diagnostic tests to intercept primary heart involvement in systemic sclerosis: clinical associations from the SPRING-SIR registry: Antonio Tonutti1|2, Francesca Motta1|2, Rossella De Angelis3, Valeria Riccieri4, Silvia Laura Bosello5, Fabio Cacciapaglia6, Veronica Codullo7, Giacomo De Luca8, Francesca Ingegnoli9, Dilia Giuggioli10, Clodoveo Ferri10, Marco Matucci-Cerinic8, Carlo Selmi1|2, Maria De Santis1|2 | 1Department of Biomedical Sciences, Humanitas University Pieve Emanuele, Milan, Italy; 2Rheumatology and Clinical Immunology, IRCCS Humanitas Research Hospital Rozzano, Milan, Italy; 3Università Politecnica delle Marche Ancona, Italy; 4Università degli Studi di Roma La Sapienza Roma, Italy; 5Università Cattolica del Sacro Cuore Roma, Italy; 6Università degli Studi di Bari Aldo Moro Bari, Italy; 7Reumatologia, Fondazione IRCCS Policlinico San Matteo Pavia, Italy; 8Università Vita-Salute San Raffaele Milano, Italy; 9Università degli Studi di Milano, Italy; 10Università degli Studi di Modena e Reggio Emilia, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Jul. 28];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2366
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


