
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:20:007 | Mind the rebound: ctx dynamics after denosumab discontinuation and zoledronate rescue in patients with postmenopausal osteoporosis or with cancer treatment-induced bone loss
Federico Aldegheri1, Francesca Ruzzon1, Matteo Appoloni1, Giovanni Adami1, Davide Gatti1, Maurizio Rossini1, Angelo Fassio1, Ombretta Viapiana1 | 1Università di Verona, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
109
Views
Authors
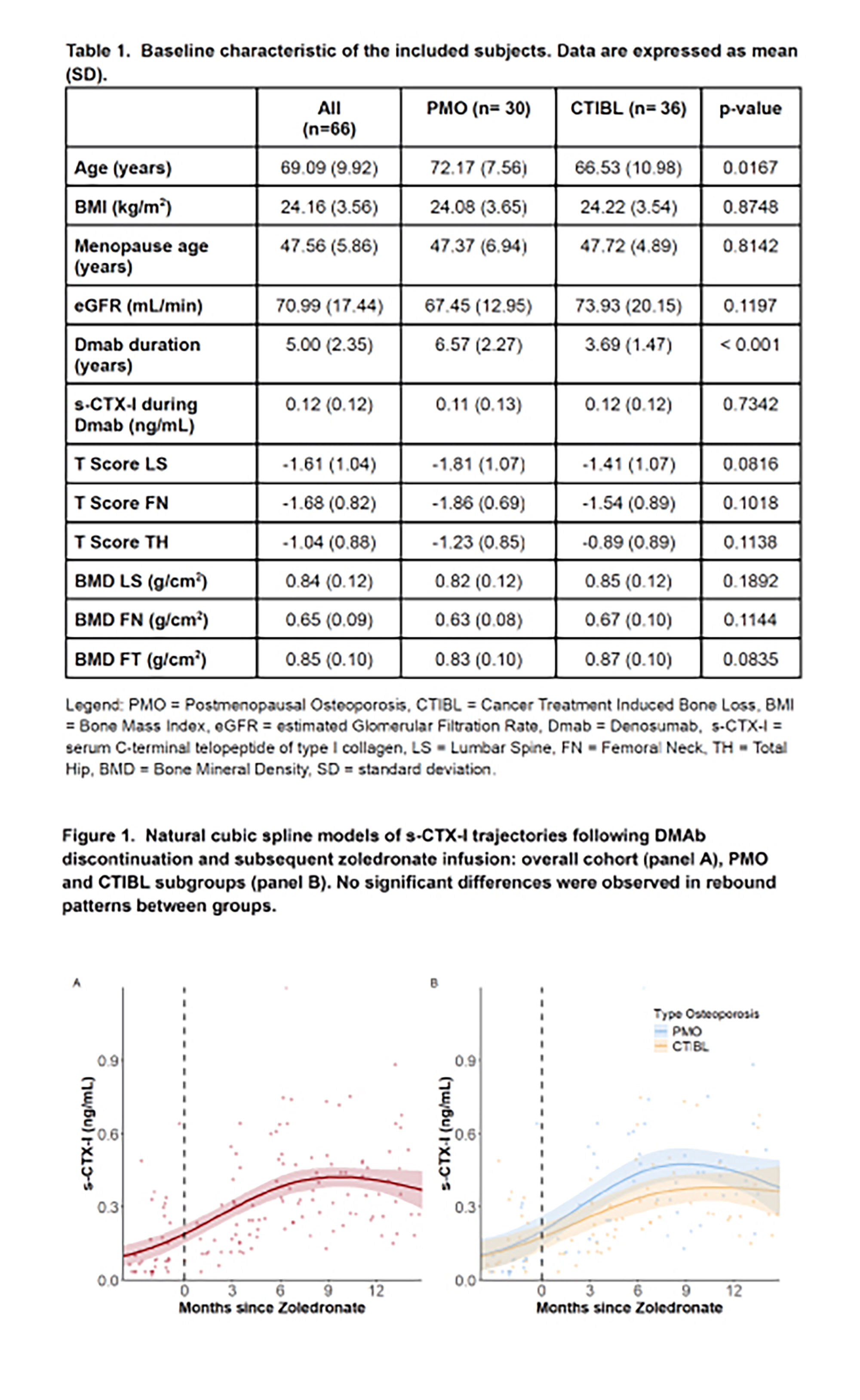
Materials and Methods. We analyzed longitudinally collected serum samples assayed for Collagen Type I C-Telopeptide (s-CTx-I) from women who discontinued Dmab and who received a single Zoledronate infusion (“day 0”) administered exactly six months after their last Dmab dose. Subjects who received Dmab either as treatment of PMO or CTBIL were included. The reasons for Dmab discontinuation were: achievement of a low fracture risk (as measured by the DEFRA algorithm) for PMO, and discontinuation of endocrine adjuvant therapy (ET) for CTBIL plus low fracture risk. To model s-CTX-I trajectories over time, we initially fitted a linear mixed-effects model, subsequently added polynomial terms (quadratic and cubic), and ultimately employed a natural cubic spline mixed-effects regression to achieve the best fit, using two internal knots (the first at day -30—approximately one month before zoledronate administration—and the second at day 180). An interaction term between time and subgroup (PMO or CTBIL) was added to assess potential between-group differences. Models were adjusted for age and duration of prior Dmab exposure. To determine the best fit, models were compared through Akaike information criterion (AIC), Bayesian information criterion (BIC), and Bayes factor.
Results. Thirty women with PMO and thirty-six with CTIBL were enrolled. CTIBL patients were younger and had a shorter duration of Dmab compared to PMO patients, while baseline bone mineral density and s-CTX-I levels were comparable (table 1). Among the models tested, the spline model provided the best fit compared to linear and polynomial models to describe s-CTX-I trends. Specifically, s-CTX-I trajectories exhibited a significant non-linear rise during the first six to nine months post-zoledronate, followed by a plateau (figure 1A). No significant treatment by subgroup interaction was observed (interaction p = ns; figure 1B), even after adjustment for age or Dmab duration.
Conclusions. Following denosumab discontinuation, and despite subsequent zoledronate administration, s-CTX-I levels rise rapidly and nonlinearly, peaking within six to nine months, with a comparable pattern observed between the PMO and CTBIL subgroups. Furthermore, ET discontinuation does not appear to offer substantial protection against the rebound associated with denosumab withdrawal. Close monitoring of s-CTX-I levels in the early phase after denosumab discontinuation seems crucial to detect early increases in bone turnover and to appropriately adjust sequential therapies.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:20:007 | Mind the rebound: ctx dynamics after denosumab discontinuation and zoledronate rescue in patients with postmenopausal osteoporosis or with cancer treatment-induced bone loss: Federico Aldegheri1, Francesca Ruzzon1, Matteo Appoloni1, Giovanni Adami1, Davide Gatti1, Maurizio Rossini1, Angelo Fassio1, Ombretta Viapiana1 | 1Università di Verona, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Aug. 1];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2342
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


