
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:15:214 | Identification of SLE patients with high-levels Type 2 SLE through the polysymptomatic distress scale (PSD): correlations with other PROs and differences in clinical phenotypes in a multicentric cohort
Micaela Fredi1|2, Giorgia Gozzoli1|2, Federica Bonaso1|2, Silvia Ebe Della Pina1|2, Claudia Barison1|2, Irene Lorenzini2, Anna Mattiuzzo2, Raffaele Pericotti2, Marcelo Neto3, Sofia Avedo4, Clàudia Oliveira4, Luis Sousa Ines3, Franco Franceschini1|2 | 1Rheumatology and Clinical Immunology, ASST Spedali Civili of Brescia, ERN-ReCONNET Center, Brescia, Italy; 2Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy; 3Rheumatology Department, Centro Hospitalar Universitário de Coimbra - ULS Coimbra, Coimbra, Portugal; 4Rheumatology Department, ULS Aveiro, Aveiro, Portugal
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
45
Views
Authors
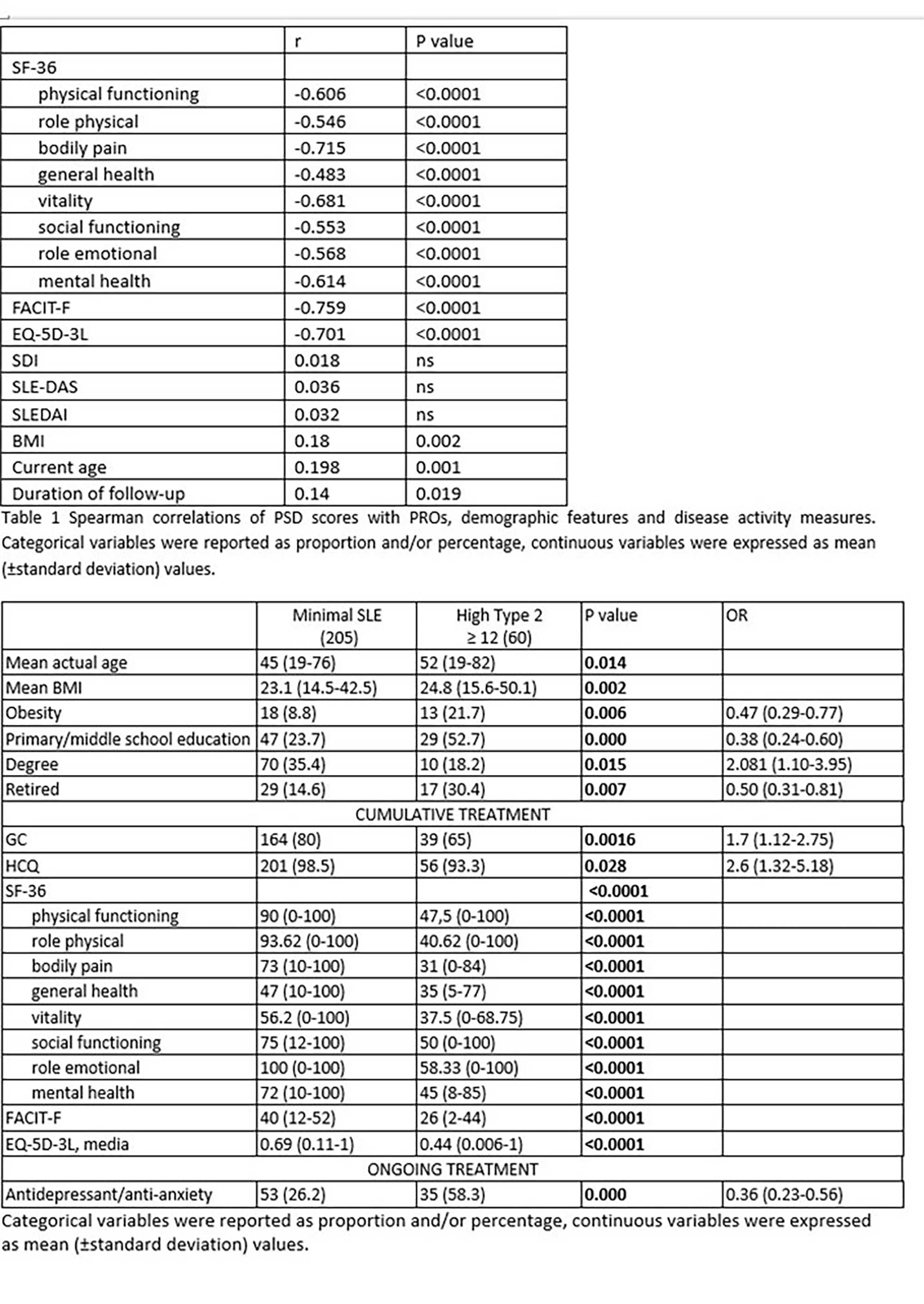
Materials and Methods. Adult SLE patients consecutively followed in two Lupus Clinic from March-July 2024 were included. High-level Type 2 is defined as PSD equal-more than 12(2), whereas high Type 1 symptom severity as a SLEDAI-2K more than 6(3). 4 groups were defined: high Type 1, high Type 2, both high Type 1-Type 2 symptoms (Mixed SLE) and no Type 1-Type 2 symptoms (Minimal SLE)(3). Fatigue was assessed through FACIT-Fatigue, quality of life with EQ-5D-3L and SF-36.
Results. The study included 277 patients, (256 women), Caucasian in 92.8%,with a median age at enrolment of 46 years (min-max 19-82). 30(12.7%) patients had a diagnosis of fibromyalgia. At the last evaluation mean SLEDAI-2K was 1.48 (±1.77); 184(80.3%) met the criteria for DORIS remission. We reported a mean PSD of 7.99(±6.08) and, as shown in table 1, PSD score strongly correlated negatively with other PROs but not with disease activity or damage scores. Moreover, a significant positive correlation was found with BMI and disease duration. PSD equal-more than12 was found in 63 (22.7%) patients, and we divided our cohorts in 4 groups: minimal SLE (205,73.9%), high-level Type2 SLE (60,21.6%), high-level Type 1 (9,3.2%) and 3 mixed. Comparison between patients with and without high-level Type 2 is reported in table 2. No differences were found in cumulative clinical manifestations, disease activity or damage and ongoing SLE treatment, whereas patients with higher PSD were older, with a higher BMI and more frequently had a primary/secondary education. Moreover, they had a worse performance in all PROs.
Conclusions. High level Type 2 SLE symptoms occurred in nearly 25% and its occurrence was not related to classic disease manifestation or objective disease activity, but with other features as weight, age, concomitant depression/anxiety. Moreover, PSD performance strongly correlates with other PROs and has the advantage of being completed in a short time and therefore its use in daily practice could be more feasible. References (1)Pisetsky DS et al. Arthritis Care Res (Hoboken). 2019 (2)Wolfe F et al Semin Arthritis Rheum 2016; (3)Eudy AM et al. Lupus. 2024
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:15:214 | Identification of SLE patients with high-levels Type 2 SLE through the polysymptomatic distress scale (PSD): correlations with other PROs and differences in clinical phenotypes in a multicentric cohort: Micaela Fredi1|2, Giorgia Gozzoli1|2, Federica Bonaso1|2, Silvia Ebe Della Pina1|2, Claudia Barison1|2, Irene Lorenzini2, Anna Mattiuzzo2, Raffaele Pericotti2, Marcelo Neto3, Sofia Avedo4, Clàudia Oliveira4, Luis Sousa Ines3, Franco Franceschini1|2 | 1Rheumatology and Clinical Immunology, ASST Spedali Civili of Brescia, ERN-ReCONNET Center, Brescia, Italy; 2Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy; 3Rheumatology Department, Centro Hospitalar Universitário de Coimbra - ULS Coimbra, Coimbra, Portugal; 4Rheumatology Department, ULS Aveiro, Aveiro, Portugal. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Jul. 27];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2327
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


