
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:11:170 | When Paget Meets Inflammatory Back Pain: A Diagnostic Dilemma Between Bone Remodeling and Spondyloarthritis
Marco Capodiferro1, Giuseppe Lopalco1, Giulia Righetti2, Gianluigi Della Corte2, Patrizia Suppressa2, Florenzo Iannone1, Fabio Cacciapaglia1|2 | 1Unit of Rheumatology, Department of Precision and Regenerative Medicine, Area Jonica DiMePRe-J, University of Bari, Italy; 2Miulli General Hospital Acquaviva - Department of Medicine and Surgery, LUM F. De Gennaro University, Casamassima, Bari, Acquaviva delle Fonti, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
141
Views
Authors
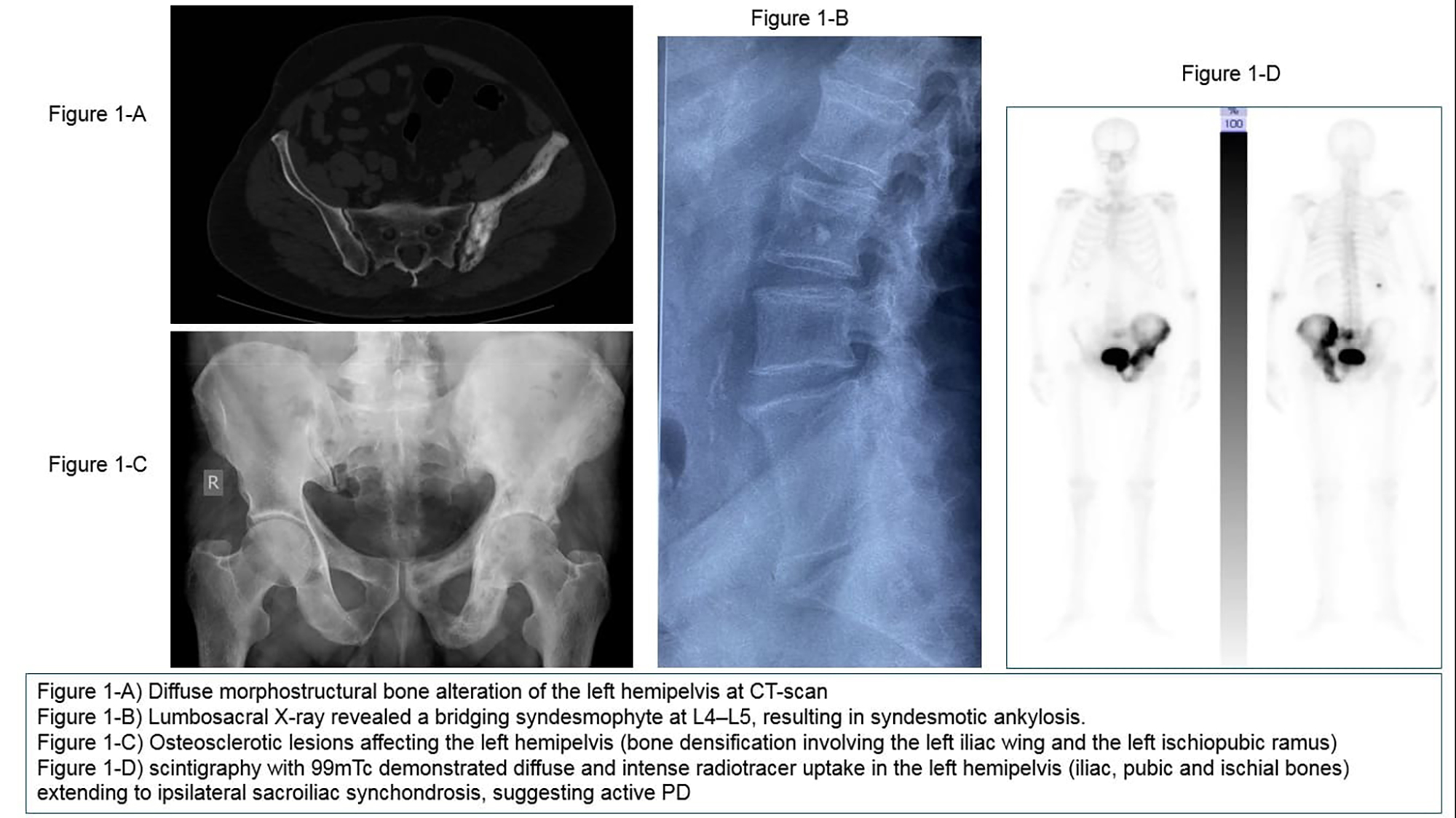
Case Presentation. A 72-year-old man presented with low back pain and lower limb myalgias, primarily localized to the left groin, radiating anteriorly along the thigh to the popliteal fossa. The patient had received diagnosis of PD 12 years earlier after a CT-scan performed for renal pain, with accidental evidence of sclerotic lesions in the left hemipelvis (Fig.1A) without skeletal symptoms. At our physical examination, he had focal tenderness over the left sacroiliac synchondrosis and iliac wing; thoracic hyperkyphosis and limited lumbar spine mobility were noted. X-ray revealed bridging syndesmophyte at L4–L5 (Fig.1-B) and sclerotic lesions involving the left ischiopubic ramus (Fig.1-C). Lab tests showed elevated alkaline phosphatase (429 U/L). Bone scintigraphy with 99mTc demonstrated intense radiotracer uptake in the left hemipelvis and ipsilateral sacroiliac synchondrosis (Fig.1-D).
Discussion. The coexistence of PD and axSpA is rare but documented. Both conditions may involve the axial skeleton, particularly the sacroiliac joints and spine, and the prevalent disease may be difficult to be evidenced. Because both diseases frequently involve the pelvis and lumbar spine, their symptoms and radiological findings may overlap, particularly regarding chronic low back pain and spinal stiffness. PD is characterized by excessive osteoclastic activity followed by disorganized osteoblastic bone formation, resulting in cortical thickening and altered trabecular architecture. Elevated alkaline phosphatase and focal scintigraphy uptake are sensitive markers of disease activity. Radiographically, lesions appear as well-defined sclerotic areas, typically sparing the joint line. Ankylosing spondylitis (AS), the prototypic form of axSpA, is a chronic inflammatory disease that affects entheses, leading to syndesmophyte formation and progressive fusion of sacroiliac joints and vertebral bodies, often resulting in a bamboo spine appearance. In rare cases inflammatory bony bridges (syndesmophytes) can provide a pathway for the contiguous spread of Paget's lesions, facilitating the development of pagetic vertebral ankylosis as uncommon potential complication.
Conclusions. This case illustrates the diagnostic complexity in distinguishing low back pain due to PD from that due to axSpA especially when sacroiliac and vertebral changes coexist. A precise differential diagnosis is essential, as treatment strategies differ substantially. While elevated ALP and focal scintigraphic uptake support active PD, the presence of syndesmophytes raises suspicion of coexisting axSpA. Furthermore, age at disease onset and NSAIDs response may help in clinical suspicious, but a comprehensive clinical and radiological evaluation is crucial to guide management and prevent complications such as vertebral ankylosis, spinal cord compression or neoplastic evolution.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:11:170 | When Paget Meets Inflammatory Back Pain: A Diagnostic Dilemma Between Bone Remodeling and Spondyloarthritis: Marco Capodiferro1, Giuseppe Lopalco1, Giulia Righetti2, Gianluigi Della Corte2, Patrizia Suppressa2, Florenzo Iannone1, Fabio Cacciapaglia1|2 | 1Unit of Rheumatology, Department of Precision and Regenerative Medicine, Area Jonica DiMePRe-J, University of Bari, Italy; 2Miulli General Hospital Acquaviva - Department of Medicine and Surgery, LUM F. De Gennaro University, Casamassima, Bari, Acquaviva delle Fonti, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Jul. 29];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2312
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


