
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:11:165 | Clinical mimicry and therapeutic challenge: A Case of Rapidly Progressive Mixed Connective Tissue Disease
Elena Maria Di Virgilio1, Elisabetta Chessa2, Valentina Ibba2, Cosimina Matulli2, Jessica Sorgia1, Andrea Pace1, Matteo Piga1|2, Alberto Cauli1|2 | 1Università degli studi di Cagliari-Reumatologia, Cagliari, Italy; 2Struttura complessa di Reumatologia- AOU Cagliari, Cagliari, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
114
Views
Authors
Materials and Methods. A 60-year-old woman presented with sudden-onset, rapidly progressing symptoms within a two-month: Raynaud's phenomenon (RP), dysphagia, dyspnoea, cervical muscle weakness and weight loss. Physical examination revealed microstomia, microcheilia, sclerodactyly, diffuse skin thickening, alopecia and muscle weakness (MRC scale: 2/5 neck, 4/5 legs).
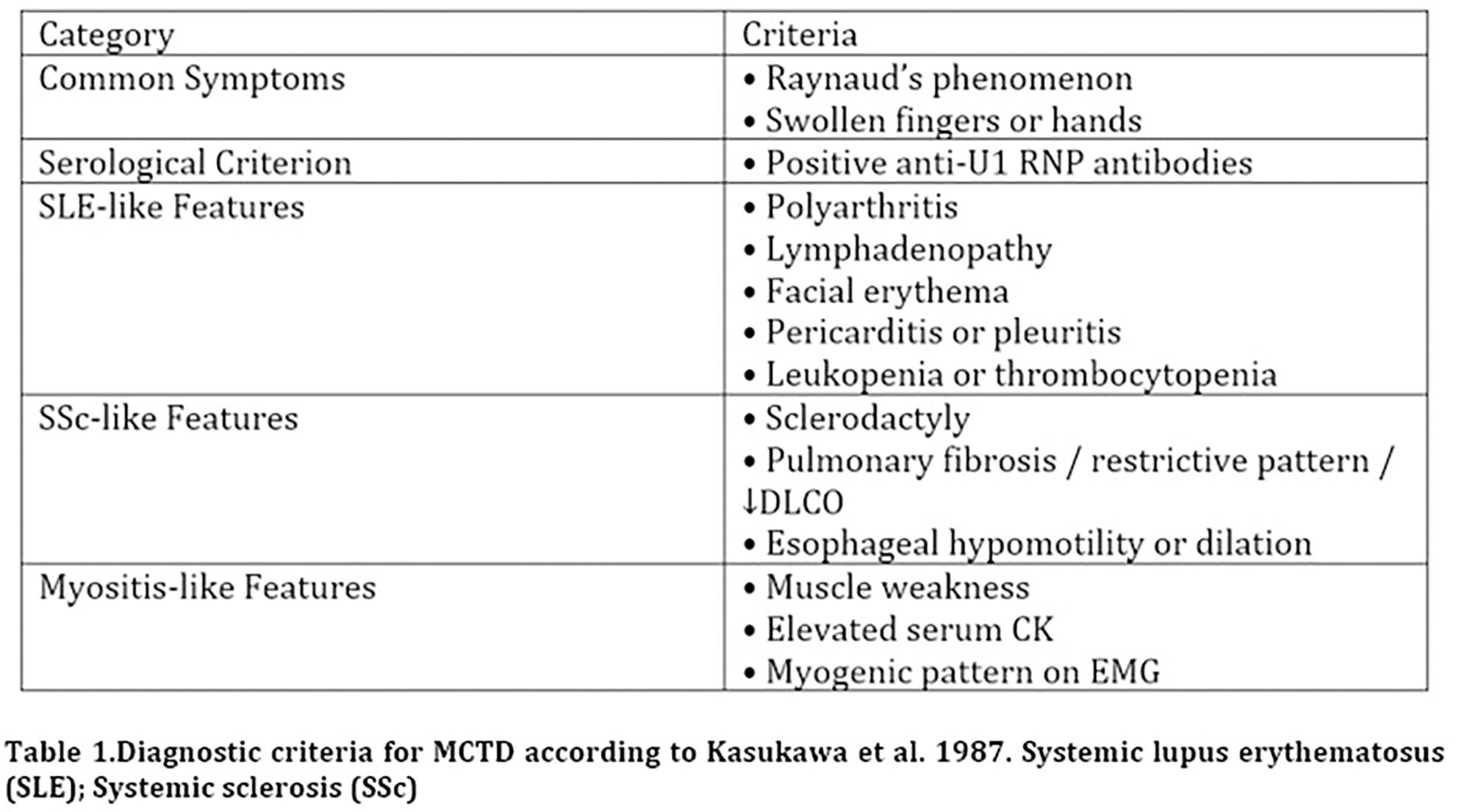
Results. Labs tests revealed elevated inflammatory markers, microcytic anemia, C3 54 mg/dl (>90), CPK 1087 U/L, troponin 2800 ng/ml, ANA 1:320 (speckled pattern) with anti-U1RNP (217) positivity. Moreover, capillaroscopy showed scleroderma pattern. CT of chest revealed reactive lymphadenopathy in the cervical-thoraco-abdominal area and pleural effusion. Pulmonary function testing was deferred due to the patient's severe clinical status. Elevated troponin (up to 3580) prompted serial echocardiography and cardiac MRI, which excluded myocarditis. Electromyography revealed sensory-motor axonal polyneuropathy and findings suggestive of inflammatory myopathy. Finally, cervical MRI revealed muscle inflammation while barium swallow demonstrated mild dilation of the distal esophagus and delayed gastric emptying. The patient met Kasukawa’s criteria (table1): the serological criterion, both common criteria (RP and scleredema), and seven disease-specific criteria: for SLE (lymphadenopathy, pericarditis/pleuritis), SSc (sclerodactyly and esophageal hypomotility), and myositis (muscle weakness, elevated serum CPK levels, and a myogenic pattern on electromyography). We performed a rescue therapy including methylprednisolone 125 mg/day, a lower dose than expected (1g/die) due to the renal crisis risk, Immunoglobulin (0,4 mg/kg/die x 5 days) and Rituximab 1g. Due to an intercurrent SarsCov2 infection, the second dose of rituximab was not administered, the remaining immunosuppressive therapy (Mycophenolate mofetil) was postponed, and the patient was treated with antiviral therapy using Remdesivir. Moreover, because of high-dose corticosteroid treatment and the disabling impact of the disease, the patient presented psychotic episode characterized by hallucinations, which required both antipsychotic medication and psychological support.
Conclusions. This case highlights how rapidly progressive MCTD can represent a major therapeutic and management challenge due to its acute onset, mimicking features of other connective tissue diseases and complications, arising from both the disease and treatment, such as immunosuppression-related risks (infections) and steroid-induced psychosis.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:11:165 | Clinical mimicry and therapeutic challenge: A Case of Rapidly Progressive Mixed Connective Tissue Disease: Elena Maria Di Virgilio1, Elisabetta Chessa2, Valentina Ibba2, Cosimina Matulli2, Jessica Sorgia1, Andrea Pace1, Matteo Piga1|2, Alberto Cauli1|2 | 1Università degli studi di Cagliari-Reumatologia, Cagliari, Italy; 2Struttura complessa di Reumatologia- AOU Cagliari, Cagliari, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Jul. 27];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2311
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


