
62nd National Congress of the Italian Society of Rheumatology
Vol. 77 No. s1 (2025): Abstract book of the 62th Conference of the Italian Society for...
PO:10:141 | A Case Study: Navigating the VEXAS Syndrome Mimickers
Erika Montabone1, Richard Borrelli1, Nicolò Rashidy1, Fabiana Giannoccaro2, Giuseppe Guida2, Federico Itri3, Renato Carignola4, Simone Negrini1, Stefania Nicola1, Luca Lo Sardo1, Iuliana Badiu1, Federica Corradi1, Ambra Bonvicino5, Maurizio Balbi6, Luisa Brussino1 | 1SCDU Immunologia e Allergologia, AO Mauriziano, Dipartimento di Scienze Mediche, Università degli Studi di Torino Torino, Italy; 2SSD Asma grave, malattie rare del polmone e fisiopatologia respiratoria, AOU San Luigi Gonzaga Orbassano, Italy; 3SCDU Medicina Interna ad indirizzo Ematologico, AOU San Luigi Gonzaga Orbassano, Italy; 4SCDU Medicina Interna, Scleroderma Unit, AOU San Luigi Gonzaga Orbassano, Italy; 5SCDU Dermatologia, Città della Salute e della Scienza di Torino Torino, Italy; 6SCDU Radiodiagnostica, AOU San Luigi Gonzaga, Dipartimento di Oncologia Orbassano, Italy
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 18 March 2026
93
Views
Authors
Materials and Methods. We present the case of a 65-year-old man initially diagnosed with psoriatic arthritis and demonstrated ANA positivity. He showed a poor response to methotrexate, TNF-alpha, and IL-17 inhibitors. Later development of biopsy confirmed panniculitic prompted a re-evaluation of the diagnosis, leading to the consideration of systemic lupus erythematosus and subsequent treatment with hydroxychloroquine and dapsone. Over time, he developed unexplained macrocytic anaemia.
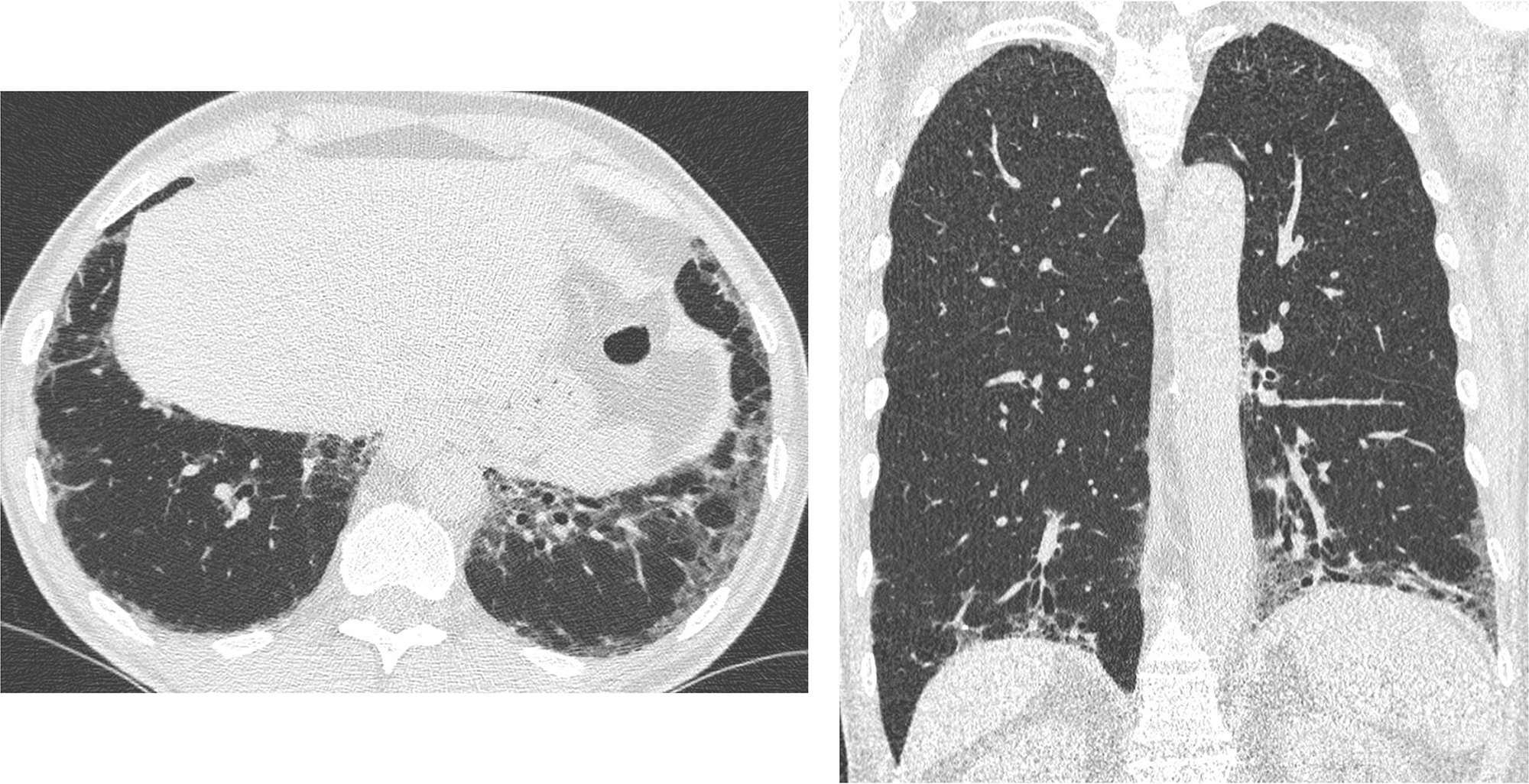
Results. Initial investigations excluded emolysis, folate or B12 deficiency and dapsone-related toxicity. Bone marrow analysis revealed mild dyserythropoiesis without overt dysplasia. Due to the onset of a dry cough, a chest HRCT scan was performed, revealing lower-lobe predominant ground-glass opacity with traction bronchiectasis, consistent with non-specific interstitial pneumonia (NSIP). The clinical presentation met the criteria for interstitial pneumonia with autoimmune features. A second bone marrow analysis using NGS identified pathogenic somatic mutations in TET2 and ZRSR2, while sequencing of the UBA1 gene was negative. MMF was introduced, partially controlling joint, skin, and pulmonary symptoms.
Conclusions. This case highlights a diagnostic dilemma involving the coexistence of autoimmune and autoinflammatory features with clonal haematopoiesis. TET2 and ZRSR2 mutations suggested a link with age-related clonal haematopoiesis or an evolving myeloid neoplasm; however, the criteria for myelodysplastic syndrome (MDS) were not met. Although UBA1 sequencing was negative, the clinical overlap with VEXAS syndrome warrants consideration of broader VEXAS-like. This case emphasizes the importance of considering immunological and genetic factors in patients with clonal hematopoiesis of indeterminate potential. This reinforces the importance of considering mutations in genes like TET2 and ZRSR2 within the context of autoimmune and inflammatory disorders, highlighting the complexities discussed in the interplay between clonal hematopoiesis and autoimmune diseases.
Downloads
Download data is not yet available.
Citations




How to Cite
1.
PO:10:141 | A Case Study: Navigating the VEXAS Syndrome Mimickers: Erika Montabone1, Richard Borrelli1, Nicolò Rashidy1, Fabiana Giannoccaro2, Giuseppe Guida2, Federico Itri3, Renato Carignola4, Simone Negrini1, Stefania Nicola1, Luca Lo Sardo1, Iuliana Badiu1, Federica Corradi1, Ambra Bonvicino5, Maurizio Balbi6, Luisa Brussino1 | 1SCDU Immunologia e Allergologia, AO Mauriziano, Dipartimento di Scienze Mediche, Università degli Studi di Torino Torino, Italy; 2SSD Asma grave, malattie rare del polmone e fisiopatologia respiratoria, AOU San Luigi Gonzaga Orbassano, Italy; 3SCDU Medicina Interna ad indirizzo Ematologico, AOU San Luigi Gonzaga Orbassano, Italy; 4SCDU Medicina Interna, Scleroderma Unit, AOU San Luigi Gonzaga Orbassano, Italy; 5SCDU Dermatologia, Città della Salute e della Scienza di Torino Torino, Italy; 6SCDU Radiodiagnostica, AOU San Luigi Gonzaga, Dipartimento di Oncologia Orbassano, Italy. Reumatismo [Internet]. 2026 Mar. 18 [cited 2026 Jul. 27];77(s1). Available from: https://www.reumatismo.org/reuma/article/view/2309
Copyright (c) 2026 The Author(s)


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


