
PO:37:257 | Giant cell arteritis debuting with aortic involvement: the importance of integrated diagnostics in fever of unknown origin
Alessandro Gratton1, Giovanni Striani1, Luisa Occhipinti1, Stefania Sacco1, Enrico Pegolo2, Luca Quartuccio1 | 1Rheumatology Clinic and 2 Institute of Anatomical Pathology, Department of Laboratory Medicine, University of Udine, Hospital “Santa Maria della Misericordia”, Udine, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background: giant cell arteritis (GCA) is the most frequent large vessel vasculitis, affecting both male and female patients older than 50 years old. Opposite to the cranic involvement (common carotid arteries and their branches) that may debut with headache and visus loss, the extra-cranic involvement (aorta and its branches) is more subtle, leading to a delayed diagnosis, causing the development of aneurisms and dissections [1-3]. Usually, these are late disease complications (after 10 years) but can be found even at diagnosis [1-3].
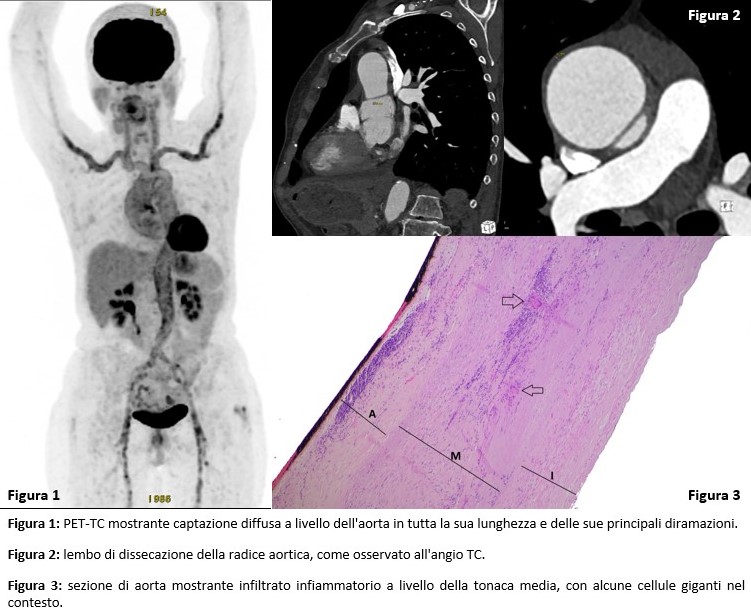
Case report: a 68-year-old woman, ex-smoker, comes to visit because of a 4-month history of daily fever (up to 38.5°C) with shivers and night sweats, myalgias, fatigue and weight loss. Blood tests showed high neutrophil and platelet count, with persistent inflammation (CRP 35 mg/L). To rule out an occult infection, the patient had been thoroughly screened with blood cultures, urine cultures, treponemic tests, which all came back negative. Being affected by a fever of unknown origin (FUO), the patient was admitted to our Clinic to undergo further testing from which no sign of autoimmunity emerged. Given the development of a persistent frontal headache, even though no other arteritis symptoms were present, an ultrasonographic study of the temporal, axillary, and carotid arteries was performed, showing no halo sign. Because of the persistence of fever and inflammation without explanation, a PET-CT and an echocardiography (to rule out infective endocarditis) were performed and, since GCA was still highly suspected, a temporal artery biopsy was scheduled. PET-CT (Figure 1) showed an intense FDG avidity along the full length of the aortic wall and the carotid and axillary arteries while the echocardiography found a dilation of the aortic root with valve insufficiency and no sign of endocarditis. Granulomatous inflammation suggesting GCA was found in the biopsy specimen of the temporal artery. The aortic dilation was studied performing a CT angiography that confirmed the enlargement of the aortic root and arch and showed a focal dissection 4 cm wide (Figure 2). Glucocorticoid therapy was immediately started and tapered for 8 weeks, alongside tocilizumab, leading to the resolution of fever and inflammation. In the meantime, heart surgeons successfully performed a replacement of the aortic arch. Histological analysis of the aortic wall confirmed the GCA diagnosis (Figure 3).
Conclusions. PET-CT and temporal artery biopsy should always be a part of the FUO diagnostic work-up, even when signs or symptoms suggesting GCA are absent. They turn out to be crucial to timely diagnose the disease and may help early identify severe and potentially fatal complications like aneurisms and aortic dissections that, despite being more frequent in the late course of the disease, can also be found at its debut4. This has important therapeutic and prognostic implications.

Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


