
Impact of ultrasonography detected quadriceps calcific tendinopathy on pain and function in patients with primary knee osteoarthritis
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Accepted: 14 May 2021
Authors
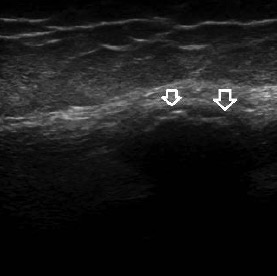
Calcific tendinopathy is most commonly seen around the shoulder joint. Only a few cases of quadriceps calcific tendinopathy (QCT) were reported. This study compares pain, function, clinical examination results, and ultrasonographic findings among primary knee osteoarthritis (KOA) patients with or without ultrasonography-detected QCT. A cross-sectional study was conducted on 214 patients with knee OA. Ultrasonography (US) of knee joints was performed according to the EULAR guidelines. Kellgren-Lawrence radiographic grading was used to score OA. Pain and functional status were assessed using the visual analog scale (VAS), the Health Assessment Questionnaire-II (HAQ-II), and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). QCT was detected in 50 out of 428 knees (11.6%), i.e. in 46 out of 214 patients (21.49%). Most cases of QCT were detected in the following sites: 36 in the vastus lateralis (72%), 10 in the vastus intermedius (20%), and only 4 in the vastus medialis (8%). QCT was found mainly in advanced KOA stages: 44 cases of QCT were found in patients with grade 4 KOA and 6 cases in grade 3 KOA. The presence of QCT showed a statistically significant association (p<0.05) with VAS, HAQ-II, WOMAC subscales, synovitis, and effusion detected by US. In knees with ultrasound-detected QCT, ultrasonographic features of CPPD were found in 31 knees (62%). QCT was found in cases with advanced KOA and mainly with ultrasonographic findings of CPPD disease. QCT could be considered an independent poor prognostic finding regarding pain, functional activity, and response to NSAIDs.
Downloads
Citations






